Back in July, partners from the NACP project came together in Stratford, London to host the final learning festival event to take place as part of the 3 year project.
Community members, volunteers, local groups, organisers and people from across the UK came together to celebrate 3 years of the project and discuss all things Co-Production.
We kicked off the day with a group meal, sharing delicious Indian street food from Ghara – something we felt was important to do given the theme of the day was sharing our cook book which included ‘recipes’ for Co-Production.
During the first part of the event, people were invited to share their own recipes (or methods) for Co-Production, after which the project team began to present ideas and examples of projects rooted in Co-Production.
Towards the late afternoon our marketplace was opened up. Pop up activities took place throughout the venue, from collaborative collage, to community reporting, an interactive recipe wall and even a human library, people got stuck into some Co-Production themed activities.
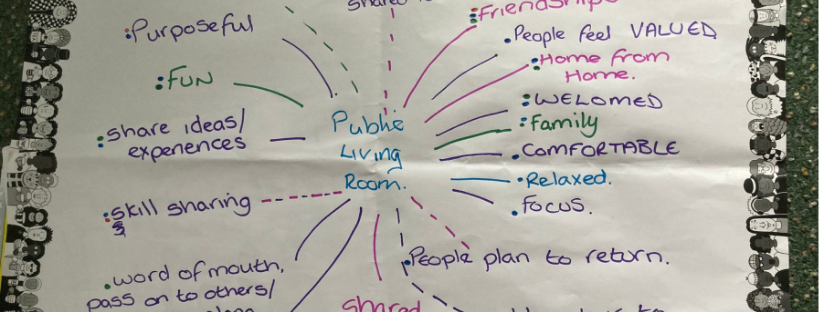
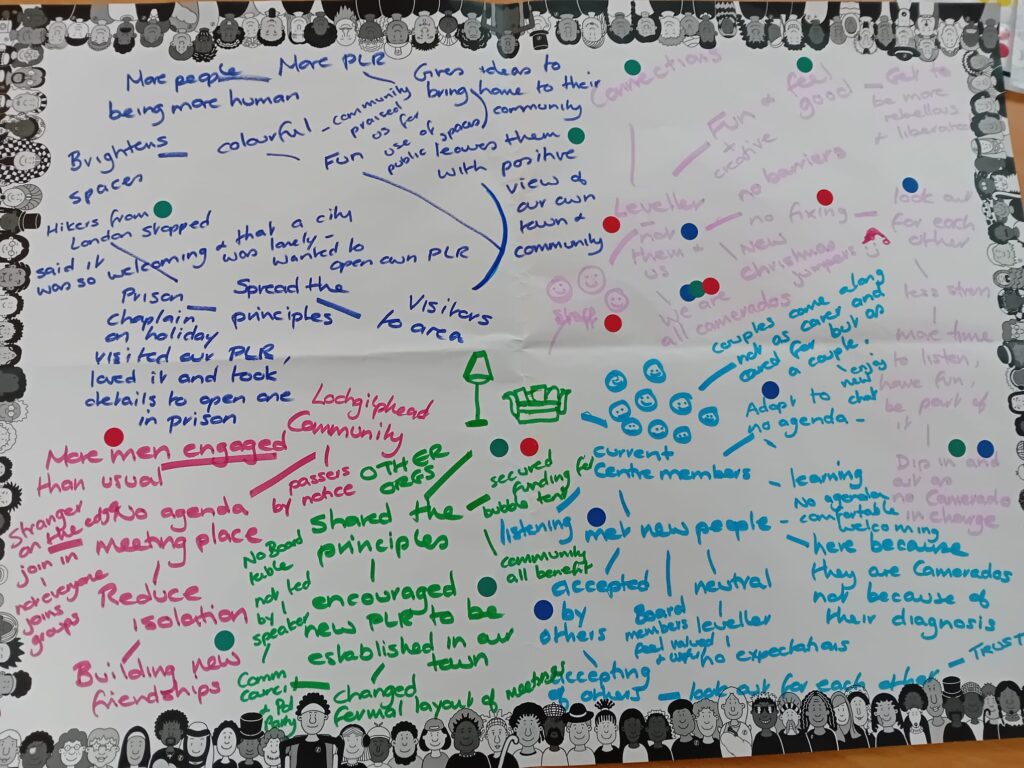
Camerados came along and generously hosted our very own Public Living Room, which was complimented perfectly by our resident DJ and biscuit dunking competition.
Another significant part of the day was the launch our Co-Production Cook Book. This cookbook includes recipes from some of the fantastic people who adventured with us over the last three years, from Greater Manchester, the West Midlands and North East London.
We invite you to use these recipes freely in your communities and see where they take you! Please be sure to credit the authors when you do, in the spirit of Co-Production. Follow the link above to access the full cook book.
A huge thank you goes out to the project team, Ideas Alliance, Camerados, and everybody who came along to the event – your contributions and support made it a truly amazing day.
We’re now in the process of reflecting on the project, if you’ve been involved and would like to share your experiences with us – get in touch with Georgia to find out how georgia@peoplesvoicemedia.co.uk